MEXICO CITY (AP) — Mexico announced Monday that several top U.S. advisers on border and immigration issues will meet with Mexican officials on Tuesday to discuss migration and development in Central America.
The talks come as a surge of migrants has hit the U.S. southern border. The trip to Mexico will include Roberta Jacobson, the White House’s lead adviser on the border, and Juan González, the National Security Council’s senior director for the Western Hemisphere.
The White House said Jacobson, a former U.S. Ambassador to Mexico, will go there Monday “to engage with Mexican government officials to develop an effective and humane plan of action to manage migration.”
Roberto Velasco, Mexico’s director for North American affairs, said the talks will focus on the two countries “joint efforts for secure, safe and regulated migration,” and plans to provide economic development in southern Mexico and Central America so people won’t come under pressure to migrate.
The White House said Gonzalez will then go on to Guatemala, to “meet with Guatemalan government officials, as well as representatives from civil society and non-government organizations to address root causes of migration in the region and build a more hopeful future in the region.”
Also among the U.S. officials is Ricardo Zúñiga, who was named Monday as Special Envoy for the Northern Triangle, which includes El Salvador, Guatemala, and Honduras — three of the countries sending the most migrants to the United States.
The State Department said Zuñiga will “coordinate closely with the National Security Council staff on the administration’s comprehensive efforts to stem irregular migration to the United States and implement President Biden’s multi-year, $4 billion to address root causes of migration in Central America.”
Since Biden’s inauguration, the U.S. has seen a dramatic spike in the number of people encountered by border officials. There were 18,945 family members and 9,297 unaccompanied children encountered in February — an increase of 168% and 63%, respectively, from the month before, according to the Pew Research Center.
U.S. border patrol officials had encountered more than 29,000 unaccompanied minors since Oct. 1, nearly the same number of youths taken into custody for all of the previous budget year, according to administration officials.
Mexico announced restrictions last week on nonessential travel across its southern border with Guatemala and Belize “to prevent the spread of COVID-19,” and sent hundreds of immigration agents and National Guard to the southern border to clamp down on crossings.
Mexico did not explain why the measure was announced now, more than a year after the start of the pandemic, but it came on the same day the U.S. confirmed it will send 2.5 million doses of the AstraZeneca coronavirus vaccine to Mexico.
Officials say migrant traffickers are encouraging people to make the trip by claiming the U.S. border is open to migrants, while Biden administration officials have stressed that the border is not open.
Mexico has cooperated with U.S. efforts to stem the flow, while stressing that the problem can only be solved by addressing the root problems of poverty and joblessness that lead many to migrate. Mexico has proposed massive investment to promote economic development in those areas
SAN JUAN, Puerto Rico (AP) — Puerto Rico’s government on Monday was granted access to more than $900 million in federal education funds less than two weeks after reopening dozens of public and private schools for the first time since the pandemic began.
The $912 million is available immediately, but the U.S. Department of Education will work with Puerto Rico officials to identify how the money would be used to address the academic, social, emotional and mental health needs of students in the U.S. territory, according to a spokeswoman for Jenniffer González, the island’s congressional representative.
The money comes as Puerto Rico struggles to recover and rebuild from the 2017 hurricanes Irma and Maria and a string of strong earthquakes that began in late 2019 and destroyed or damaged dozens of schools in the island’s southern region. Then the pandemic hit, forcing hundreds of private and public schools to close for nearly a year as teachers and students alike struggled with power outages and spotty or nonexistent internet connections amid virtual learning.
“Our students have been through too much,” said Gov. Pedro Pierluisi. “They deserve a semblance of normalcy.”
Pierluisi authorized the reopening of certain public and private schools this month to some students, but scarce attendance was reported amid fears of contagion as less than 100 of Puerto Rico’s 858 public schools reopened nearly two weeks ago for the first time in a year. For now, only kindergarteners, special education students and children in first, second, third and 12th grades are allowed to return to school. They attend in-person classes only twice a week and are dismissed before noon.
The release of federal education funds comes as Puerto Rico pursues a new relationship with the administration of U.S. President Joe Biden, with local officials hopeful that funding delays common under the former Trump administration will dissipate.
“The department understands the urgency to access vital federal education funds to meet the needs of Puerto Rican students who are experiencing compounded trauma,” U.S. Secretary of Education Miguel Cardona said in a statement.
A robbery has occurred tonight in Kawaha Point, Rotorua. Police were called to the report of a robbery in Bellvue Rd at 7.50pm, a media spokeswoman said. “Police are speaking with the victim and working to establish what took…
Hon. Mark Brantley, Premier of Nevis and Senior Minister of Health in the Nevis Island Administration after taking his first dose of the Oxford-AstraZeneca COVID-19 vaccine on February 25 at the Charlestown Health Centre in Nevis.
I’m bashing my head as well,” says Devi Sridhar. It is January 2021, and the Florida-born, Edinburgh-based professor of global public health is looking back on the pandemic year, marveling and despairing at opportunities lost.
From early last winter, Sridhar has been among the most vocal critics of the shambolic U.K. response — urging categorically more pandemic vigilance, which she believed might have yielded a total triumph over the disease, a cause that has picked up the shorthand “Zero COVID.” “This is where I started,” Sridhar says. “An elimination approach to the virus. My mind never went, ‘Oh, we should treat this like flu.’ It started off with, like, ‘We treat it like SARS until I see evidence otherwise.’”
In 2003, SARS had been eliminated after only 8,000 infections; its biggest foothold outside Asia was in Canada, which reported just a few hundred suspected cases. With COVID, Sridhar says, “I was following the response in China. They went into lockdown. You saw New Zealand pivoting that way and then Australia after.”
But not the U.K., where an erratic series of scientific advisories pushed the government first to embrace a target of herd immunity, then to backpedal, but not enough. Sridhar describes those advisories with retrospective horror, an inexplicable preemptive surrender by the public-health apparatus.
“Basically, going back to January, they’d be like, ‘China’s not going to control it; 80 percent of the population is going to get it; all efforts to contain it are going to fail; we have to learn to live with this virus; contact tracing and testing make no sense; this is going to be everywhere; right now we need to build up hospitals’ — which they didn’t even do. But they really didn’t think it was stoppable,” she says.
“And then all of a sudden you started to see, in February, South Korea stopping it, Taiwan stopping it, and China stopping it. Then, in March, New Zealand. And then Australia. And then there’s this realization of, ‘Oh, wow. Actually, it is controllable.’”
At the beginning of March, South Korea was averaging more than 550 new daily confirmed cases, compared with just 53 in the U.K. At the end of the month, South Korea had 125; the U.K. was at 4,500 and climbing. “In the UK we have had nine weeks to listen, learn and prepare,” Sridhar wrote angrily in the Guardian, berating the British regime for failing to establish basic systems for supplies, testing, and contact tracing.
“Countries such as Senegal were doing this in January,” she wrote. “We had a choice early on in the UK’s trajectory to go down the South Korean path,” but instead the country was at risk of sleepwalking from small failures into giant ones. “We must race to make up for the time lost during two months of passivity,” Sridhar concluded. Of course, the country didn’t, and now its death toll measures in the six figures. Sound familiar?
“I mean, the U.K. was consumed with Brexit,” Sridhar says now. “The U.S. had Trump. To them, this is something happening somewhere else across the world. And they just want to ignore it as long as they could.” As the pandemic progressed, both exhausted countries flipped from denial to capitulation, choosing to treat almost any caseload plateau as an opportunity to relax, no matter how high a level of ongoing spread it represented.
“It was like, ‘We’re gonna have a great summer and holidays,’” she says, laughing ruefully. “Can you believe it? Last summer, I was up on panels with Tory politicians where they’re saying, ‘You’re safer flying to Greece or to Spain than being in the U.K. because they have lower rates than us.’ And they are 100 percent serious! It’s like it’s a basic human right, to have a holiday and go abroad, and we can’t possibly take it away.
Everyone was saying elimination was impossible. You still hear it, right? ‘Impossible, it’s impossible.’ Which is kind of the choice that we’ve made here. Elimination is just too difficult.”
Sridhar is pointing her finger at British authorities, but in her diatribe you could comfortably substitute for the U.K. almost any nation in Europe. In its broad strokes, the picture has been the same in Belgium and France and Italy and the Czech Republic, too, in Portugal and Poland, Sweden and Switzerland and Spain, even Germany and the Netherlands, and dozens of other countries across the Continent.
From the spring panic through the fall surge, pandemic policy differed nation to nation, but failure was general all across Europe. Aside from the three Nordic outliers of Finland, Norway, and Iceland, no European state has managed the coronavirus well by global standards — or by their own much higher ones.
For decades, the richest nations of the world had told themselves a story in which wealth and medical superiority offered, if not total immunity from disease, then certainly a guarantee against pandemics, regarded as a premodern residue of the underdeveloped world.
That arrogance has made the coronavirus not just a staggering but an ironic plague. Invulnerability was a myth, of course, but what the pandemic revealed was much worse than just average levels of susceptibility and weakness. It was these countries that suffered most, died most, flailed most. Gave up most easily, too, acquiescing to so much more disease that they might have been fighting a different virus entirely.
For nearly the entire year, the COVID epicenter was not in China, where the pathogen originated, or in corners of South Asia or sub-Saharan Africa, where limited state capacity and medical infrastructure seemed, at the outset, especially concerning, but either in Europe or the United States — places that were rated just one year ago the best prepared in the world to combat infectious disease.
This fact, though not unknown, is probably the most salient and profound feature of what has been a tremendously uneven pandemic with the world’s longtime “winners” becoming by far its biggest losers. The gold-standard responses were those in East Asia and Oceania, by countries like South Korea, New Zealand, and Australia — countries that saw clearly the gravest infection threat the world had encountered in a century and endeavored to simply eradicate it within their borders. Mostly, they succeeded. When it mattered most, no nation in what was once grandly called “the West” even really bothered to try.
The opera audience on October 18, 2020, in Wuhan, China. Photo: Getty Images
The virus is the virus,” says Gregg Gonsalves, the former AIDS activist turned epidemiologist, now a MacArthur “genius” with a public-health position at Yale. “There’s ways to stop it, and then there’s …” He pauses for a moment. “It has its own logic and its own trajectory.”
In the U.S., the story of the pandemic year has been dominated by the character of the president who presided over it so ineptly, often with such indifference it seemed he was rooting for the disease. But the problem with assigning Donald Trump all, or even most of, the blame for America’s suffering is that the country’s failure isn’t unique.
In fact, before the arrival of vaccines, the American experience of the coronavirus was not exceptional but typical — at least among those European nations it typically considers its peers. And as the New Year has brought a new administration, experts in fields from public health to economics have grown more comfortable acknowledging that catastrophe was much bigger and deeper than the denier-in-chief and indeed much more “normal” than Americans outraged or mourning are likely to understand.
The metric of deaths per capita is crude, obscuring issues of demography and comorbidity, but by this basic standard the U.S. has suffered less than the U.K., Portugal, and the Czech Republic. It sits clustered with a number of other European nations — Italy, Spain, France — near the E.U. average. The South American average is just below.
None of these countries, save Brazil, had presidents or prime ministers who so callously downplayed the threat of the disease as Trump, or who tried to suppress testing, or who held indoor political rallies during a local surge. “But that’s not to say that in some counterfactual scenario where someone else was president, we would not be having difficulty,” Natalie Dean, a biostatistician at the University of Florida, told me. “There are only so many tools at our disposal.”
Francois Balloux, an infectious-disease epidemiologist and computational geneticist at the University College of London, goes further. “It’s not obvious that different measures taken in different places have clearly led to different outcomes,” he says. “There’s a lot of idiosyncrasy, and I think it’s simplistic to say that the countries that have controlled or eliminated the virus did things extremely differently.
If you just list, for instance, the interventions that places like New Zealand or Australia have implemented, they’re not drastically different — in stringency nor duration — than in some other places. The country that had the strictest lockdown for longest in the world is Peru, and they were absolutely devastated. I think the slightly depressing message,” Balloux says with a sigh, “is that there is not just a set of policies that will bring success and can just be applied to any place in the world.”
This is not how the disease has been regarded by most American liberals, who’ve tended to see COVID as a straightforward management challenge, in which the pandemic can be “solved” through science-first policy and dutiful compliance — a perspective that has given the pandemic features of a morality play, in which matters of social distancing and masking become tests of executive and personal virtue that determine the course of the disease.
But local disgust is not exclusively an Anglo-American phenomenon. “If you read the national press from any country, be it Germany or Switzerland or France, whatever, there’s a strong feeling in most places that, actually, the situation is the worst locally,” says Balloux. The historian Adam Tooze, at work on a rapid-fire account of 2020, argues that this intuition is less an insight into pandemic policy than it is a reflection of national narcissism.
“It is clear that both the U.K. and the U.S. will almost perforce frame what’s happened in terms of narratives of national crisis,” he says. “But in general I just don’t think it’s all that helpful either in the U.K. or the U.S. to talk in terms of a specific national failure.”
Even within America, the coronavirus hasn’t precisely cooperated with the spirit of determinism. The highest per capita death rate, for instance, is not found in Texas but in New Jersey. Through the devastating fall surge, a poll found that 90 percent of American adults were wearing a mask “sometimes, often, or always.”
Close contacts in states with heavy restrictions were not dramatically higher than in laissez-faire places, and even draconian lockdowns produced, typically, plateaus or slow caseload declines, not rapid descent to zero. There are, within the U.S., a few relative success stories—Hawaii, notably, has registered almost no excess mortality. But death rates in Florida, proudly one of the loosest states, are hardly any higher than they are in California, self-flagellatingly one of the strictest.
None of this is especially surprising to epidemiologists, who have spent whole careers swimming in viral uncertainty. The rest of us are left to shout in bafflement, How can this be? “I took this question for like two months, basically, to every expert I know in California,” says Soumya Karlamangla, the reporter at the Los Angeles Times most deeply embedded in the Southern California pandemic, who’d become somewhat obsessed with trying to explain the contrast, seemingly paradoxical, with Florida.
“I’d just ask them over and over. And the thing I kept hearing from these experts was something I was kind of surprised by. They don’t know. They just don’t have a good explanation.” My experience has been largely the same. When I asked Shane Crotty, a virologist at the La Jolla Institute for Immunology in San Diego, if he had a sense of why the country’s worst autumn surge had come in Southern California, a place without a traditional autumn, his short answer was: “No, I don’t.”
This is not to say that policy and behavior don’t matter — only that containing a novel disease we understand incompletely is not as simple as hitting the “Science” button. The mitigation measures on which the country has focused the most — masking, social distancing, school closures, restaurant restrictions — are curve-benders, not firewalls. And many of the factors playing a much larger role in shaping the spread of the pandemic fit much less comfortably in a technocrat’s shoulder bag or a liberal’s scolding moralism.
A partial list: There is stochasticity, better known as chance, driven in part by superspreader dynamics, whereby the vast majority of new cases are produced by a thin slice of existing infections and most disease chains simply die out. There is demography, with the skew of lethality so dramatic that many of the world’s younger countries have almost no death toll. There is distribution of comorbidities throughout the population. There is geography, with islands enjoying obvious advantages, and with communities at higher latitudes apparently more at risk, perhaps due to the salubrious effects of sunlight.
There is a country’s relationship to its own borders, and who its neighbors are, and its position in the networks of travel and commerce. There is climate, with temperature and especially humidity appearing to shape national outcomes much as they’ve shaped some seasonal rhythms of the disease within countries.
There is air conditioning — whether you have it, and what kind. There is what Crotty described to me as a version of the “hygiene hypothesis” — the possibility that regular exposure to pathogens generally might train your immune system like it does your gut biome. There is the catchall of “cultural forces,” covering everything from multigenerational living and employment structures to cheek-kissing and handshakes.
I could go on: residential density, blood type, vitamin D, ICU capacity, proximity to bats. But any time you try to put a finger on a single, dominant factor, the disease slips away, defying reductive models and suggesting counterpoints and counterfactuals: Japan is old, Brazil is largely tropical, England is an island, and there’s hardly any air conditioning in France.
And even beyond all of those factors, with relative impacts of unclear scale, there is what the controversial Stanford epidemiologist John Ioannides recently called the “chaos” of the disease — the seemingly random, and still mysterious, dynamics of spread, even beyond stochasticity, which can be at least mathematically modeled.
The recent collapse in American case numbers, for instance, came right after the New Year, in the middle of what the country had just been warned — by epidemiologists and the new president, in his inauguration speech — would likely be the pandemic’s darkest season. Looking back, you could find a few lonely voices suggesting winter would be calmer than autumn. But the CDC aggregates and showcases 26 pedigreed models predicting the near-term course of the disease.
On January 18, only two of the 26 showed the dramatic case decline the country experienced by February 1 as being within what’s called the 95 percent confidence interval. In other words, 24 of the 26 models said what ended up happening over just the next two weeks was, more or less, statistically impossible. The other two gave it, at best, a sliver of a chance.
And yet for all that mystery, one distinct pattern stands out, with national outcomes falling into three obvious clusters whose basis and cause may be investigated for decades as the most significant feature of the whole global pandemic.
In Europe, North America, and South America: nearly universal failure. In sub-Saharan Africa and South Asia: high caseloads and low death rates, owing largely to the age structure of populations. In East Asia, South-East Asia and Oceania: inarguable success. You can compare countries within these clusters, and wonder why Canada has outperformed the U.S. or why Uruguay has outshone Argentina, why Iran suffered so much or how Japan, which never locked down and never tested all that widely, succeeded so brilliantly.
But the differences in outcomes between the groups of nations are far greater than those within them, so much so that they appear almost as the burn scars of entirely different diseases. By damage, the coronavirus has not been a “Chinese flu” but a western malady, and if you were making guesses about how a particular nation has fared, by far the most significant piece of data would be where on the planet it was located.
Take Germany. Since the beginning of the pandemic, Angela Merkel has been celebrated as a beacon of rational leadership — a technocrat with a doctorate in quantum chemistry, presiding calmly over an unprecedented crisis, with a citizenry often stereotyped as compliant, orderly, respectful of science.
To judge by death, Germany has indeed outperformed the U.S., with fewer than 900 per million citizens, compared to our more than 1,600. But New Zealand, to pick one counterexample, has registered just over five per million. That is, for every Kiwi per million who died, so did 162 Germans. And 298 Americans.
New Zealand has natural advantages — it’s small, it’s an island, it’s got national health care; when the disease arrived and containment mattered most, it happened to be summer; there’s an inspiring prime minister, and social trust is high. (The country’s approach has been described as “treat every case like a murder,” and indeed, the entire city of Auckland recently shut down in response to a single family’s positive test.)
Which of these factors, or what combination, is decisive? Nearby Australia is a much larger nation, with a divisive media powered by Rupert Murdoch, and a Trump- or at least Boris-like leader. It has bigger airports and plenty of A/C. You might expect Australia to look a lot more like the U.S. or U.K. But its death rate is under 36 per million — less than one-50th the American rate. They had crowds at much of the Australian Open, you might’ve seen. Of course, the players had to quarantine for weeks before getting on the court.
In East Asia, though, nobody envies the Antipodes. In Taiwan, the death rate is a minuscule 0.42 per million. The European Union performed, on average, 3,000 times worse. Cambodia hasn’t reported a single COVID death all year, and while it is probably fair to assume that the official data don’t tell the full story, what is most startling across East and Southeast Asia — an incredibly heterogeneous region, with wealthy nations and poor ones, democracies and authoritarian regimes, national health-care systems and patchwork networks — is just how consistent the story is. In Vietnam, there have been 0.36 deaths per million, in China 3.36.
In Singapore, the number is around five; in South Korea, it is close to 32; in Japan, in many ways the best contrast for the aging and wealthy nations of Europe and North America, it’s about 67. Again, you can doubt some of these numbers, the Chinese figures especially. But in the U.K., remember, the level is north of 1,800.
III.
An outdoor concert on February 13 in Wellington, New Zealand. Photo: Mark Tantrum/Getty Images
What few people realize is that, yes, the virus originated in China, but the true focus of the epidemic that spread to the world was actually in northern Italy,” says Balloux, who has observed the pandemic from London. “We think it happened in Asia first. But the countries that were seeded most massively, the countries that were hardest hit, were not the countries that had the most contact with China. Many of the countries that were hardest hit were the countries that had contact with northern Italy.”
You can plausibly chalk this up to some combination of chance, “natural” or cultural factors, and Asia’s experience with SARS and MERS, which functioned as useful dry runs — exposing public-health shortcomings and acculturating local populations to dramatic preventative measures. Taiwan and Singapore, Balloux says, closed up “before the virus was really there,” perhaps fast enough to entirely eliminate local transmission. In Italy, by contrast, “by the time they realized they had a serious outbreak, it was far, far too late.”
As early as the spring, the former Portuguese diplomat Bruno Maçães was suggesting that indifference in Europe and the U.S. reflected a kind of pandemic Orientalism. When China put Wuhan into lockdown, he told me, the intervention was doubly and catastrophically discounted by the NATO states.
The disease was dismissed as a culturally backward outgrowth of wet markets and exotic-animal cuisine, and the shutdown was seen not as a demonstration of extreme seriousness but as a sign of the reflexive authoritarianism of the Chinese regime (and the imagined servility of its population). In fact, China was not in the habit of quarantining entire metropolises.
“It was a huge shock for them,” Tooze says now. “With SARS, they hardly did a shutdown at all … We should have said, ‘Oh my God, it’s Wuhan — 11 million super-affluent people. Jesus, that’s what we’re going to have to do.’” But that “would have required the West to really own what was going on in China,” he says. “I think that’s the big problem. You would have had to have said to people in the West, ‘Look, this is going to look crazy — we are going to stop JFK and Heathrow in their tracks. But look what they’re doing in China.’”
An early, globally coordinated pause on travel, the virologist Florian Krammer says, would have likely averted catastrophe even if it had only lasted a few weeks — a shutdown that, in retrospect, would qualify as impossibly modest, given the billions of people sheltering in place in the spring and the trillions of dollars disgorged from treasuries and central banks since to support them. “But right now I think there’s a huge gap between the reality of globalization and our ability to actually apprehend what that means,” Tooze says.
Tooze is an economic historian whose last major work was an authoritative history of the 2008 financial crisis and its global fallout, and for him, the echoes are unmistakable. “One of the ways in which we deal with the radical nature of the experiment that we’re running — massive economic growth at the global scale, involving most of 7.8 billion people — is that we live in a state of denial.
We don’t actually take in what this implies most of the time at lots of different levels. And of course there are Cassandras, there are people whose job it is to say, ‘No, no, no, it’s all connected.’ But they’re siloed off and placed in, as it were, cognitive bubbles, whose relationship to actual key decision-making is arbitrary.” And in general, he says wryly, “I’ve been impressed by the Sinophobia that it has revealed in Europe.”
But it wasn’t just Sinophobia. Even after the disease arrived in Europe, nearly every western nation chose to play wait-and-see — hoping they wouldn’t have to intrude on the lives of their citizens and economies, and trusting that, if they needed to, they could simply play catch-up without paying anything like a true pandemic price. Italy’s outbreak didn’t inspire immediate responses elsewhere on the Continent, and neither did Spain’s.
In the U.S., cases in Washington State didn’t inspire leaders in New York to move, and though the horrible New York spring did inspire lockdowns in many “virgin” states, they were often short-lived, unaccompanied by real public-health preparation, and brutal enough for residents and politicians both that they made later pandemic measures harder to enact. Once the disease did come, officials tended to make the same mistake — ratcheting up restrictions as the disease worsened and ratcheting them down as it dissipated. In almost every venue, life-as-usual proved too expensive, or too difficult, or too protected by interested parties to disrupt.
When the efforts came, they weren’t just late but inadequate. Lockdowns dominated debate over pandemic policy, but failures on testing, contact tracing, and quarantine were much more notable. In April, the Nobel economist Paul Romer suggested screening every American every two weeks — about 25 million tests each day.
The country barely ever cracked 2 million. In the U.K., in February, it was estimated contact tracers could manage a total of five new cases each week. Five. In response, Boris Johnson promised a “world-beating” contact-tracing system, then delivered one where less than half of close contacts of new patients were even reached by the NHS, and perhaps as few as 11 percent of those who were reached actually chose to self-isolate in response to exposure.
In the U.S., when contact tracers called, hardly anyone bothered to pick up the phone.
“If you look at last spring, many of the European countries were doing well,” says Gonsalves, the epidemiologist. “And last summer people took their foot off the accelerator and decided that they would reopen.” This was “basically capitulation,” he says. “We gave up on eradication or elimination early on. I don’t think it was ever on the table, and it’s certainly not on the table now. By the time we get to the spring, I don’t think anybody was thinking about it in any real terms. I never felt like anybody was driving the car.”
Gonsalves has spent much of his academic career, he says, focused on “what we called the social determinants of health, everything that’s around you that keeps you healthy: housing, access to food, care in your old age, et cetera.” At the outset of the pandemic, those were a wreck in many of these countries, especially America, with outrageous health disparities across populations exacerbated by a threadbare social-welfare state.
“We’ve been told that the government is our problem, but the point is health care is a public good, not a private commodity,” he says, and one nontrivial aspect of pandemic performance was how shallow, or how deep, local willingness to fund even non-medical support proved to be. “But this is not just about the structure of social welfare, health care, and the will of the state,” he adds. “It’s about human behavior and decisions that were made about relaxing restrictions before anybody was near out of the woods, before we even knew we had vaccines.
Some of that human behavior, around the globe — it’s not necessarily a structural issue. It’s tied to human nature and how people respond to the pandemic outside the systems of governance and the state. How do you change human behavior? I don’t know.”
“The problem,” Balloux agrees, “is that you have to deal with humans. They might like doing things; they might tell you they do things and they might do other things. I think people might have complied better if there was a real feeling that it could be very useful. But I think a large part of the population in Europe felt there’s not a chance the virus could have been eliminated locally.” He adds, “I say, rightly so.”
“Clearly, the West was betting on a magic bullet,” Tooze says. “Developing the vaccine has to be understood holistically as part of our reaction, if there’s any kind of rationale behind that reaction at all. It was a part of our strategy individually and collectively — fundamentally, we’ve all basically been expecting the vaccine to arrive. Because without that, it’s pretty difficult to kind of figure out what the hell any of us really thought we were doing.”
IV.
The Australian Open on February 18 in Melbourne, Australia. Photo: Daniel Pockett/Getty Images
On March 13, 2020, Mike Ryan, WHO’s executive director of health emergencies, took the podium at a Geneva press conference and delivered in just a minute what is, to me, probably the most chilling and illuminating speech of the entire pandemic. Asked what lessons from a career fighting outbreaks of Ebola were called to mind by the arrival of COVID-19, Ryan replied with terse, cinematic force. “What we’ve learned through the Ebola outbreaks is you need to react quickly. You need to go after the virus. You need to stop the chains of transmission. You need to engage with communities very deeply — community acceptance is hugely important. You need to be coordinated, you need to be coherent.”
When it came to this pandemic, he said, speaking in a clipped Irish lilt, the lessons were the same: “Be fast. Have no regrets. You must be the first mover. The virus will always get you if you don’t move quickly.” He continued, “If you need to be right before you move, you will never win. Perfection is the enemy of the good when it comes to emergency management. Speed trumps perfection. And the problem in society we have at the moment is everyone is afraid of making a mistake, everyone is afraid of the consequence of error. But the greatest error is not to move. The greatest error is to be paralyzed by the fear of failure.”
Ryan’s speech was delivered as an admonition, but it may as well have been an indictment. As Peter Baldwin documents in his forthcoming comparative history of the pandemic, Fighting the First Wave, speed was probably the most significant factor in determining national outcomes, and just about every nation in the West failed to move quickly enough.
With the exception of Japan, whose light pandemic remains something of a mystery even within the context of the “Asian miracle,” all of the successful national campaigns resemble each other in the speed and intensity of response, and all of the failures share a similar reluctance to move preemptively — instead needing to be forced into action by the disease.
“I kind of come down to a kind of almost deterministic line, which is that we are dealing with an exponential or semi-exponential kind of a process,” says Tooze. “Either you control this early on, in which case the trade-offs are relatively manageable and all sorts of conventional things make sense, or you don’t and you end up in a space which really no advanced polity’s decision-making process is very good at coping with. And so then it’s really a matter of degrees of failure across the board.”
The pattern had already been established when Ryan spoke. A hundred and seven Italians were dead, and many more were infected, before the country took any measures at all to prevent spread, which it did on March 4. When Spain went into lockdown ten days later, it had more than 6,000 confirmed cases.
In France, local elections were held in person on March 15, despite there being almost 5,000 confirmed cases. In the U.K., with infections doubling every few days, 250,000 people attended the Cheltenham Festival beginning March 16. Germany shut all the way down only on March 23 with almost 30,000 cases. Officially, in the U.S., on the day of Ryan’s speech, only 51 Americans had died, but according to pandemic modeler Youyang Gu, perhaps 1.85 million had already been infected across the country.
New York hadn’t even begun to shelter in place. When the state did move into lockdown one week later, Gu estimates the national number had grown to 3.64 million. At that point, even if you had dispatched a contact-tracing army, the disease might well have been impossible to contain. The die had largely been cast, the mark of arrogance and indifference.
In June, in an early attempt to get beyond the “matter of regime type” and answer why some countries were beating COVID and others were failing, Francis Fukuyama suggested three major factors: political leadership, social trust, and state capacity. This formulation turns out to have been inadequate, or at the very least premature. Germany is led by Merkel. One of the highest levels of social trust in the world is found in much-maligned Sweden, with just under 1,300 deaths per million. No nation has more capacity for action than the U.S., as even Fukuyama acknowledged. And here the American experience is telling.
On February 11, a month before Ryan’s press conference, Anthony Fauci, Nancy Messonnier, and Ron Klain had taken the stage at an Aspen Institute panel on the novel coronavirus led by the superstar infectious-disease journalist Helen Branswell. Several times, Fauci repeated that he believed the virus was low-risk — later clarifying that it was important to communicate to the public that it was low-risk, in part to protect his own credibility and the credibility of the public-health Establishment. “To this day I do not understand why,” Branswell recently wrote. A few days after the panel, Fauci described the risk of the coronavirus to Americans as “minuscule.”
This was a time when the U.S. public-health infrastructure assuming (or even pretending to assume) a war footing might have made a meaningful difference. But at every opportunity, Fauci was counseling the opposite — calm in the face of the storm. On February 15, he told an interviewer that the flu was a bigger threat to Americans.
For another month, he was still advising against masks. It wasn’t just Fauci (whom the upstart leftist magazine The Drift recently mocked as “Dr. Do-Little” in what likely won’t be the last reconsideration of the sainted physician). New York governor Andrew Cuomo, a cable-news hero in the spring, has already come in for reconsideration, and in his self-aggrandizing pandemic memoir, he is unintentionally revealing.
“Most of all, I was concerned about public panic,” Cuomo writes, reflecting on the need to “socialize the notion of a shutdown,” ideally slowly, rather than simply imposing it. “Panic is the real enemy,” he adds. The coronavirus may not prove Cuomo’s ultimate political undoing, but his formulation may nevertheless provide the most fitting epitaph for the entire western response: that disruption was scarier and less tolerable than the disease.
By American standards, Cuomo did move quickly — putting his state in lockdown just 20 days after the first confirmed case, three times faster than Washington State or California. But he waited for cases to arrive on his doorstep to act, and even then, his first instinct was to reassure rather than disrupt. In that, he was far from an outlier.
Through the winter, the guidance from America’s public-health Establishment was clear, beamed to the public through columns and op-eds like those in the New York Times warning “beware the pandemic panic” and, in the Washington Post, arguing “we should be wary of an aggressive government response to coronavirus.” Other headlines from the time: “We Should Deescalate the War on the Coronavirus,” from Wired; “Coronavirus Is Scary, but the Flu Is Deadlier, More Widespread” from USA Today; “The Flu Is a Far Bigger Threat to Most People in the U.S. Than the Wuhan Coronavirus,” from Business Insider.
Before flu comparisons became a talking point of the pandemic-denier right, they were the reassuring focus of the Establishmentarian left. Perhaps the short-sighted and self-interested president would never have moved more quickly or more emphatically in response to a different kind of warning. But governors might have, and mayors, and the public at large. Instead, the cause of the alarm was picked up not by those in positions of social authority or with the power to enact preparatory measures but by a rogues’ gallery of outsiders and contrarians: Peter Navarro, Trump’s personal China hawk; Scott Adams, the Dilbert guy; Balaji Srinivasan, a cryptocurrency evangelist from Silicon Valley; Eric Feigl-Ding, a nutrition-focused epidemiologist then affiliated with Harvard who got a bit out over his skis in a series of panic-inducing tweets, then came in for a professional drubbing by his colleagues.
Onstage in February, Messonnier — the CDC’s coronavirus lead — seemed to be operating from the same playbook of reassurance as Fauci. She suggested that early estimates of the severity of the disease were likely too high, before acknowledging that “if the disease is transmittable by people who are asymptomatic or even just mildly symptomatic, it makes it really clear that we’re not going to be able to keep it from spreading in the U.S.” She joked, “The thing to think about in the U.S. is there’s only so much worrying you can do every day.” Later, she added, “People like responding. They don’t like preparing.”
At this point, the U.S. had 13 confirmed cases, and though the true number was certainly much higher, preparation (or even response on the South Korea model) was still possible. But Messonnier was offering her observation as a statement of deep cultural truth, one that was echoed through the seasons in comparisons between the American and European response to the pandemic and those observed in East Asia: People here would never stand for lockdowns, it was said, or surveillance-scale testing, or mandatory quarantine. In a lot of these comparisons, there were problematic invocations of “Confucian” culture and mischaracterizations of liberal democracies like Japan and Taiwan as “authoritarian.”
But then, in short order, many Americans did stand for something like lockdown. And while we never got to surveillance-scale testing or mandatory quarantine, the fact that we sheltered in place for that long, and in modified ways for almost a full year, suspending the majority of our social, romantic, professional, and educational lives in ways that would have been considered, just a month before, unthinkable, suggests that perhaps it would not have been understood as a civil-rights violation to take a rapid antigen test once a week or to pass through a temperature checkpoint to enter buildings, if it had been said to be necessary — or rather, “worth it.”
It wasn’t that these countries did nothing, because ultimately they did an enormous amount. It was that everything they did was late, unfocused, and poorly executed — at least as far as containing the actual disease was concerned. Lockdowns were supposed to be a last resort. But practically speaking, the only thing we did to make them less likely was give up.
In retrospect, it seems almost by design. At stage right at the Aspen event, beside Fauci and Messonier, was Klain, who had led the much-lauded Obama-era Ebola response team. “My overwhelming experience as the Ebola czar,” he joked, “was that I was the czar of nothing, right? Because we don’t have a command-and-control health-care system in the United States.” This made rapid preparation — even if desired — difficult.
“We have a system that’s part public and part private, that is largely state and local based. Most of the troops in Nancy’s army are state and local employees, when you get right down to it. If you’re going to have a big monitoring program, or a big contact-tracing program, that’s not going to be done by the fantastic people at the CDC; that’s going to fall on state and local government. And if we have hundreds, or thousands, of people in hospitals, those beds are going to be provided by private hospitals, public hospitals, state and local hospitals.
You know,” he said, gesturing at Fauci and Messonnier, “these two sit at the top of a federal health-care system that is not a federal health-care system. That’s not what we have in America.” Of course, there are national health systems in Canada, Mexico, England, and France, among many others, and the uniformity of failure across this heterodox group suggests that structure may have made less of a difference than culture.
“One of the common features is that we are a medical-centric group of countries,” says Michael Mina, a Harvard epidemiologist who has spent the pandemic advocating for mass rollout of rapid testing on the pregnancy-kit model — only to meet resistance at every turn by those who insisted on a higher, clinical standard for tests.
“We have an enormous focus on medicine and individual biology and individual health. We have very little focus as a group of nations on prioritizing the public good. We just don’t. It’s almost taboo — I mean, it is taboo. We have physicians running the show — that’s a consistent thing, medical doctors across the western European countries, driving the decision-making.” The result, he says, has been short-sighted calculations that prioritize absolute knowledge about everything before advising or designing policy about anything.
It’s a perspective echoed by Zeynep Tufekci, the scholar of technology who has become perhaps the most treasured “outsider” analyst of the disease and pandemic policy in the U.S. — an independent thinker who has, again and again, called out the limitations and perversities of public-health guidance on everything from masking to asymptomatic transmission to the role of aerosols and the importance of ventilation.
She recently surveyed the system’s biggest failures — including that experts sometimes misled the public on key points out of fear that advising them honestly would lead them to take more risk; that hard rules (six feet apart, for no more than 15 minutes) were offered in place of broad principles (“like Japan’s, which emphasize avoiding the three C’s — closed spaces, crowded places, and close contact”); and a preference for false certainty (“There is no evidence of human-to-human transmission”) rather than honest nuance (“There is increasing likelihood that human-to-human transmission is taking place, but we haven’t yet proven this”).
These were not narrowly American issues, or western ones—in fact, much of the problematic guidance came from the WHO. But in East Asia, countries didn’t wait for the WHO’s guidance to change on aerosols or asymptomatic transmission before masking up, social-distancing, and quarantining. “They acted fast. They acted decisively,” says Mina.
“They made early moves. They didn’t sit and ponder: ‘What should we do? Do we have all of the data before we make a single decision?’ And I think that is a common theme that we’ve seen across all the Western countries—a reluctance to even admit that it was a big problem and then to really act without all of the information available. To this day, people are still not acting.” Instead, he says, “decision-makers have been paralyzed. They would rather just not act and let the pandemic move forward than act aggressively, but potentially be wrong.”
This, he says, reflects a culture of medicine in which the case of the individual patient is paramount. In the early months of the pandemic, the “heroic” medicine of doctors trying out experimental treatments on patients may have raised the death count considerably. And at the level of public guidance, throughout America and Europe, there has been a tendency to regard anything that didn’t offer perfect and total protection against transmission as needlessly risky behavior — outdoor exercise, socializing with masks, holiday travel with a negative test in hand.
If you’re advising a single, vulnerable patient, Mina suggests, it might make sense to propose staying at home through a surge, but it’s not necessarily useful advice for everyone, and neglects to offer practical guidance for how to navigate a pandemic world in favor of an indefinite, exhausting, abstinence-only piece of quasi-propaganda. That’s not really public health, he says, it’s medicine.
And even so, the guidance that was offered wasn’t all that illuminating at the individual level — with 10,000-times higher lethality rates hidden behind vague language like “the elderly are more at risk,” or comorbidities discussed as an almost uniform additional risk, so that my kidney-patient father-in-law, for instance, didn’t know that he was significantly more vulnerable than my mother with COPD.
“Some of these discussions are not scientific,” Dean says. “It’s more holistic than that. There’s some core public-health communication that I wish had been a little more in center, coming from the harm-reduction world of HIV, acknowledging that people have a need for social interaction. Shaming doesn’t really work. It can be counterproductive, can drive activity indoors. We needed to give people safer alternatives and provide people with information about how to do it.” Some of this guidance, she says, made sense in an initial rush to respond, but the longer they went on, the more nuance and perspective should’ve been incorporated.
“Back then, people were like, ‘Okay, we can do this for a week, we can do this for three weeks.’” Only later, and somewhat quietly, did it “acquire a longer time period. And so we have to think also a bit with sustainability in mind. How do we communicate with people? What is the goal? What is the plan? Because I think there’ve been times when it felt like we were a little aimless as a country — just sort of muddling through. At least we should, you know, have a goal.” The result was considerably more pandemic fatigue than was necessary.
“People often associate public health with froofy theory and froofy ideas, but that’s not at all what real public health is about,” Mina says. “Public health is engineering systems to benefit the population in a way that is sometimes entirely at odds with medicine.
Sometimes you need to sacrifice some people for the benefit of the population as a whole. You take risks that maybe a doctor isn’t willing to take. Instead of optimizing the immunological response at the individual level” — for instance, by prioritizing a second dose of the vaccine, which for Moderna bumps efficacy from 80 to 95 percent — “you optimize the immunological protection of the population,” say by spreading out first doses to more people, each of whom get that 80 percent protection. These kinds of decisions, he says, involve trade-offs and uncertainty, of course, but waiting for perfect data is a luxury from the before times.
“Now, the number of doctors who say, about testing or anything else, ‘Well, hang on, you don’t know that …’ It’s like, no, ‘We don’t know that, but you know what? Somebody who has a trillion viral particles in the respiratory tract is probably transmitting more than somebody with a thousand.’ You know, those orders of magnitude are quite distinct. But even that question — ‘Is a trillion viral particles more transmissible than a thousand?’ — the average doctor, until they see the data that shows that somebody with a trillion viral particles is more likely to transmit to somebody than somebody with a thousand at that time, they don’t believe it.”
Again and again, in conversations about the pandemic spanning months, the metaphor that Mina returned to, with an almost uncomfortable single-mindedness, was war. “This is a national emergency, this is a war that we’re in, and instead of putting generals in positions of power, we’ve deferred to academics,” he said. “Imagine in World War II, if that was how we treated it all — that we couldn’t make a single mistake.”
The metaphor, though vivid, also suggests its own answer to the question of pandemic lethargy and indifference. “Especially in a country like the U.S., but also in the other European countries — we haven’t felt discomfort in a long time,” Mina says. “I remember saying back in February or March, ‘I don’t think the U.S. is going to fare well here,’ for no other reason than we won’t even be able to know and to recognize that something bad is happening to us.
And I think that has not abated in the United States or in Europe. We have continued to just think that something bad isn’t happening to us, and that there’s an out somewhere — that, of course we’re going to solve this next month. It’s always been one month away. And as long as the solution is always one month away, the urgency isn’t there. And I do believe that this is a symptom of a bunch of nations and societies that really haven’t had to deal with adversity on our shores in a really long time. We are uncomfortable with making the hard decisions that have to be made.
“China made really hard decisions — some could say they infringe on the rights of their population. That seems so insane to a bunch of privileged countries, that we would have allowed that kind of thing to happen on our shores. Because that would have been us admitting that something absolutely terrible was happening to us.”
Of course, there are the vaccines, delivering Americans into a new pandemic era — and perhaps turning the page so definitively on the catastrophe of the last year we fail to learn anything meaningful from it.
Never before in the history of medicine has the spread of an infectious disease been halted so early by the development of vaccines. And here, the U.S. and the U.K. are world-class, on track to deliver shots to anyone who wants them by summer. It’s the inverse of the story of pandemic containment, with two of the world’s most striking national failures delivering two of the most impressive vaccine programs.
Places that appeared as recently as a few months ago to represent perhaps an entirely new geopolitical category — what the essayist and consultant Umair Haque has called the “rich, failed state” — appear now quite enviable, especially among the Continental nations of Europe. There, vaccine rollouts have been caught up in far more red tape. Japan and South Korea are vaccinating at just a fraction of the British or American rates. “One big thing we’re learning is what it means for a country to be good at things — it’s not as unidimensional as one might’ve thought,” the economist Tyler Cowen says. “Countries are good at very different things. And it’s not all wrapped up in one happy bundle.”
But what is most impressive about the mRNA technology in the Pfizer-BioNTech and Moderna vaccines is not just how quickly they’ve arrived. It’s that the novel vaccines developed in response to the novel coronavirus herald the possibility of an entirely new era for medicine generally. These COVID-specific “platforms” could be easily adjusted for other variants or perhaps adapted into a universal coronavirus vaccine, and Moderna says that other of its mRNA tools could be used to customize new immunotherapies for cancer, among other things.
Already in clinical trials, the company is sequencing the genes of a patient’s tumor and designing personal mRNA drugs targeting that specific malignancy. In this sense, the western response to the pandemic is almost a caricature of neoliberalism: indifference to human suffering and unwillingness to disrupt the quotidian churn of a prosperous economy, combined with high-end scientific genius and capital-intensive investment by state actors in profit-oriented innovation, the fruits of which are then hoarded by the global rich (in this case, Americans).
What this all looks like a year from now remains, as a result, very much an open question, and it is striking, at this point, how little leaders have been punished. “Americans, in their lives as citizens and voters, have not rebelled against what has happened,” Cowen says.
“And you have to blame that as a more fundamental cause than whatever the government has screwed up, which is plenty.” Trump, the face of America’s pandemic incompetence, almost won reelection, falling by only a small margin in critical states. Gavin Newsom is likely to be recalled, and Andrew Cuomo is immolating in scandals both related and unrelated to his management of the pandemic, but in Texas, Greg Abbott’s approval ratings are above water, and in Florida, Ron DeSantis has gotten eight points more popular since summer.
The pattern holds abroad as well. In the U.K., Johnson’s Tories are stronger than they’ve been in more than half a year. In Mexico, with nearly 1,500 deaths per million citizens, the net approval rating of Andrés Manuel López Obrador is +33. Perhaps that is another sign of broad acquiescence to sclerosis, state failure, and political decay.
But it also complicates intuitive narratives about cultural decline, like, perhaps, the one that hangs over this essay. The vaccines may have been the only real response the U.S. managed to the new disease; they may also mark a generational biotech turning point and an end to what Cowen has long lamented as the “Great Stagnation” of American innovation and growth.
“Unless current trends change dramatically,” Fukuyama wrote in his June essay, “the general forecast is gloomy.” He was not just predicting the rise of China at the expense of the U.S. as a result of the pandemic, but considering the possible arrival of a dark timeline for liberal democracy more generally.
Nine months later, despite all the American death, the forecast is improbably sunny. The country’s GDP is now expected to grow beyond what pre-COVID economists predicted for 2021. With the CARES Act, a cruel Republican administration somewhat shockingly improvised a dramatic, if temporary, expansion of the social-welfare state, and in Biden’s $1.9 trillion COVID package, Democrats have endeavoured to almost single-handedly restore state capacity after two generations of market-based solutions and neoliberal austerity.
The legislation is projected to cut the poverty rate by a third, significantly improving those “social determinants of health” and, perhaps, restoring at least some American faith in state capacity and the ability of the government to actually attend to the needs of citizens. The question is, when the next pandemic comes, how much will it matter?
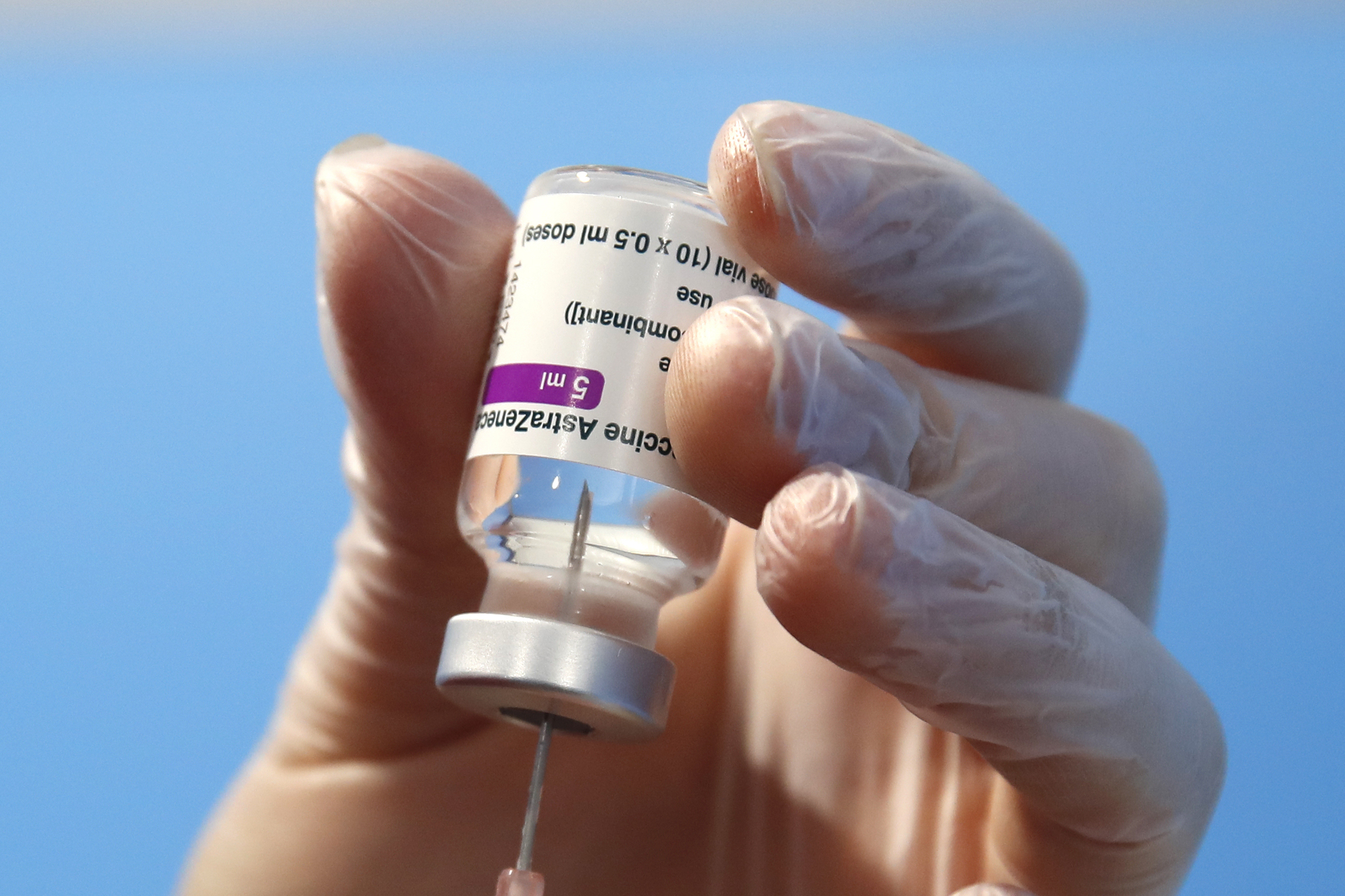
Australia's Therapeutic Goods Administration (TGA) has approved the release of more than 832,000 doses of locally-made AstraZeneca COVID-19 vaccine to be administered.
This evening the TGA confirmed it had approved the release of four batches totalling 832,200 doses.
The clearance follows last Sunday's TGA approval for the vaccine to be manufactured in Australia by CSL-Seqirus at its Broadmeadows facility.
The Australian-produced AstraZeneca vaccine has been widely touted as the solution to inoculating Australians against serious disease as a result of COVID-19.
"TGA testing of the vaccine batches in our Canberra laboratories plus review of extensive manufacturing documentation, has ensured that the locally-manufactured vaccine has the exactly the same composition and performance as the overseas-manufactured vaccine, the same quality, and is free of contaminants," the TGA confirmed in a statement.
"The TGA's clearance of the vaccine for local manufacture is a major step in Australia's response to the COVID-19 pandemic.
"We will now be able to provide secure access to large numbers of doses of a domestically-produced vaccine, with the Australian government having procured 50 million doses for delivery in the coming months."
The Australian-produced AstraZeneca vaccine will be progressively rolled out to more than 4,000 distribution points including general practices, respiratory clinics and Aboriginal Health Services.
Further approval will be required for each and every batch supplied and made in Australia.
"TGA approval is required for each and every batch of any vaccine supplied in Australia," the TGA said in a statement.
"All subsequent batches of the Melbourne-manufactured vaccine completed in the coming weeks and months will go through the same individual batch testing and release process by the TGA."
Emergency services remain at the scene of a massive three-floor building fire in Tūākau where at one point flames were shooting 30 metres into the air.At its height, huge plumes of toxic black smoke could be seen drifting…
A Melbourne man made a shock cancer diagnosis as a result of fooling around with his mates at the pub.
Mark "Cricket" Osler was enjoying a couple of beers with mates at the pub in the lead-up to Christmas.
"One of the guys was leaving and walked past me and gave me a bit of a sidekick to the backside as he left just to say, 'see you later', and it started from there," Mr Osler said.
In the weeks that followed, the 59-year-old was in excruciating pain and he was encouraged by his chiropractor to get an X-ray.
"I walked in there thinking I was going walk out with either a fracture or a bruised coccyx," Mr Osler said.
"It absolutely floored me, and I was sort of numb for about two days … I just couldn't comprehend what I'd been told."
Originally published by Māori Television An occupation has begun in the Whangārei area to put a halt to a transfer of land from the Department of Conservation to the Whangārei District Council. Pātaua South…
The rescue was part of a huge operation to evacuate hundreds of residents stranded along the Colo River in the NSW Hawkesbury region.
The State Emergency Service (SES) is warning people in Upper Colo, Lower Colo, Colo Central and Wheeny Creek after the river peaked at 11 metres this morning.
However, the threat is far from over as roads are still cut off by floodwaters.
Trucks carrying supplies and essentials such as food and medicine are on their way to nearby Windsor now conditions have eased slightly.
The SES evacuation order was initially issued about 8am, and an update at 4pm.
Residents are being urged to take only essential items such as warm clothes, medicines and insurance documents.
People who do not follow the evacuation order risked being trapped without power, food and water, the SES said.
It comes as the state faces multiple weather fronts which represent a "catastrophic" threat.
There is already major flooding at North Richmond and Windsor and it may barely recede for most of the week based on rain expected in coming days, the Bureau of Meteorology (BOM) says.
Forecasters are expecting 50mm to 100mm of rain to fall in the next 12 to 24 hours across many parts of NSW.
The BOM is warning of flash flooding bringing a serious risk to the whole northern and central coastal districts of NSW today, particularly in the Northern Rivers , Mid North Coast, Lower Hunter, Blue Mountains, and Sydney Metro regions.
It warns the extreme weather will be life threatening in some areas.
The heavy rain along the central coastal districts including Sydney Metro, Lower Hunter and Illawarra is expected to ease later today as the rain band contracts to the north and south.
The BoM has also issued warnings of damaging winds averaging 60km/h to 70 km/h, with peak gusts in excess of 90 km/h possible along the coastal fringe south of Seal Rocks from late this morning.
The SES – which has deployed about 2000 people – and other emergency services have been extremely busy over the past couple of days.
It has responded to 9000 jobs and carried out 870 flood rescues.
The BoM warned 10 million Australians were under a weather warning as two major systems collided, leaving Western Australia the only mainland state not affected.
"It may have been going for days but unfortunately this situation is far from over," the BoM said.
Warnings for heavy rain, damaging winds and heavy surf cover an area similar in size to Alaska.
Meanwhile, the Australian Defence Force will send two search and rescue helicopters to flooded areas today after NSW requested backup.
"The search and rescue choppers will be able to work through night and day and supporting personnel will be made available to make this happen," David Littleproud, the Minister for Emergency Management, said.
A short time later he took a call from NRL star Mitchell Pearce.
"Who's this sheila coming out saying something about ya?" The Knights player asked.
"We were just fooling around and she like, she like bled a little bit. It was weird," Hayne told him.
"Then she wigged out. I said nah listen you're sweet. I said f——- like my fingernail must have clipped you…"
Police had begun listening to Hayne's calls after they were alerted to the allegation by the NRL Integrity Commission, six and a half weeks after the assault in Newcastle.
"You could tell she's f—— mate just a weirdo mate, you know a young cow just carrying on," he told another caller.
Hayne was found guilty of two counts of sexual intercourse without consent yesterday.
The court heard he asked his taxi driver to wait outside the woman's home while he went inside.
The woman told the court when she realised the cab was waiting outside she decided she was not going to touch Hayne because she knew he only wanted one thing.
"My heart dropped kinda thing because I thought he had only come there for one thing."
"I think the whole time in my mind I thought this could one day turn into something."
The court heard a jail sentence is "inevitable".
Hayne was ordered to hand over $50,000 to mitigate any flight risk before his bail was continued until a sentence hearing in May.
Until then he has been ordered not to leave the Woy Woy area and to report to police daily.